 E-submission
E-submission
Search
- Page Path
- HOME > Search
Original Article
- The efficacy of treatment for hepatocellular carcinoma in elderly patients
- Han Ah Lee, Sangheun Lee, Hae Lim Lee, Jeong Eun Song, Dong Hyeon Lee, Sojung Han, Ju Hyun Shim, Bo Hyun Kim, Jong Young Choi, Hyunchul Rhim, Do Young Kim
- J Liver Cancer. 2023;23(2):362-376. Published online September 14, 2023
- DOI: https://doi.org/10.17998/jlc.2023.08.03

- 1,318 Views
- 70 Downloads
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Background/Aim
Despite the increasing proportion of elderly patients with hepatocellular carcinoma (HCC) over time, treatment efficacy in this population is not well established.
Methods
Data collected from the Korean Primary Liver Cancer Registry, a representative cohort of patients newly diagnosed with HCC in Korea between 2008 and 2017, were analyzed. Overall survival (OS) according to tumor stage and treatment modality was compared between elderly and non-elderly patients with HCC.
Results
Among 15,186 study patients, 5,829 (38.4%) were elderly. A larger proportion of elderly patients did not receive any treatment for HCC than non-elderly patients (25.2% vs. 16.7%). However, OS was significantly better in elderly patients who received treatment compared to those who did not (median, 38.6 vs. 22.3 months; P<0.001). In early-stage HCC, surgery yielded significantly lower OS in elderly patients compared to non-elderly patients (median, 97.4 vs. 138.0 months; P<0.001), however, local ablation (median, 82.2 vs. 105.5 months) and transarterial therapy (median, 42.6 vs. 56.9 months) each provided comparable OS between the two groups after inverse probability of treatment weighting (IPTW) analysis (all P>0.05). After IPTW, in intermediate-stage HCC, surgery (median, 66.0 vs. 90.3 months) and transarterial therapy (median, 36.5 vs. 37.2 months), and in advanced-stage HCC, transarterial (median, 25.3 vs. 26.3 months) and systemic therapy (median, 25.3 vs. 26.3 months) yielded comparable OS between the elderly and non-elderly HCC patients (all P>0.05).
Conclusions
Personalized treatments tailored to individual patients can improve the prognosis of elderly patients with HCC to a level comparable to that of non-elderly patients.

Case Report
- Multidisciplinary approach for hepatocellular carcinoma arising from cirrhotic liver with Budd-Chiari syndrome: a case report
- Sangmi Kim, Ji Hoon Kim, Ji Won Han, Jeong Won Jang, Jong Young Choi, Seung Kew Yoon, Pil Soo Sung
- J Liver Cancer. 2022;22(2):202-206. Published online September 20, 2022
- DOI: https://doi.org/10.17998/jlc.2022.09.17

- 1,882 Views
- 45 Downloads
-
Abstract
PDF
- Budd-Chiari syndrome (BCS) is defined by the obstruction of the hepatic venous outflow between the small hepatic veins and the junction of the inferior vena cava (IVC) with the right atrium. BCS with IVC obstruction occasionally progresses to hepatocellular carcinoma (HCC). Here, we report the case of a patient with HCC arising from a cirrhotic liver with BCS, in whom the hepatic portion of the IVC was obstructed, and who had a favorable outcome with a multidisciplinary approach and IVC balloon angioplasty.
Original Articles
- Diagnostic performance of serum exosomal miRNA-720 in hepatocellular carcinoma
- Jeong Won Jang, Ji Min Kim, Hye Seon Kim, Jin Seoub Kim, Ji Won Han, Soon Kyu Lee, Heechul Nam, Pil Soo Sung, Si Hyun Bae, Jong Young Choi, Seung Kew Yoon
- J Liver Cancer. 2022;22(1):30-39. Published online March 21, 2022
- DOI: https://doi.org/10.17998/jlc.2022.02.25

- 3,838 Views
- 131 Downloads
-
Abstract
PDFSupplementary Material
- Background/Aim
Hepatocellular carcinoma (HCC) is associated with poor prognosis, largely due to late detection. Highly accurate biomarkers are urgently needed to detect early-stage HCC. Our study aims to explore the diagnostic performance of serum exosomal microRNA (miR)-720 in HCC.
Methods
Exosomal miRNA was measured via quantitative real-time PCR. A correlation analysis of exosomal miR-720 and tumor or clinico-demographic data of patients with HCC was performed. The receiver operating characteristic (ROC) curve was used to assess the diagnostic capacity of serum exosomal miR-720 for HCC, in comparison with α-fetoprotein (AFP) and prothrombin induced by vitamin K absence or antagonist-II (PIVKA-II).
Results
MiR-720 was chosen as a potential HCC marker via miR microarray based on significant differential expression between tumor and non-tumor samples. Serum exosomal miR-720 was significantly upregulated in patients with HCC (n=114) versus other liver diseases (control, n=30), with a higher area under the ROC curve (AUC=0.931) than the other markers. Particularly, serum exosomal miR-720 showed superior performance in diagnosing small HCC (< 5 cm; AUC=0.930) compared with AFP (AUC=0.802) or PIVKA-II (AUC=0.718). Exosomal miR-720 levels showed marginal correlation with tumor size. The proportion of elevated miR-720 also increased with intrahepatic tumor stage progression. Unlike AFP or PIVKA-II showing a significant correlation with aminotransferase levels, the exosomal miR-720 level was not affected by aminotransferase levels.
Conclusions
Serum exosomal miR-720 is an excellent biomarker for the diagnosis of HCC, with better performance than AFP or PIVKA-II. Its diagnostic utility is maintained even in small HCC and is unaffected by aminotransferase levels.
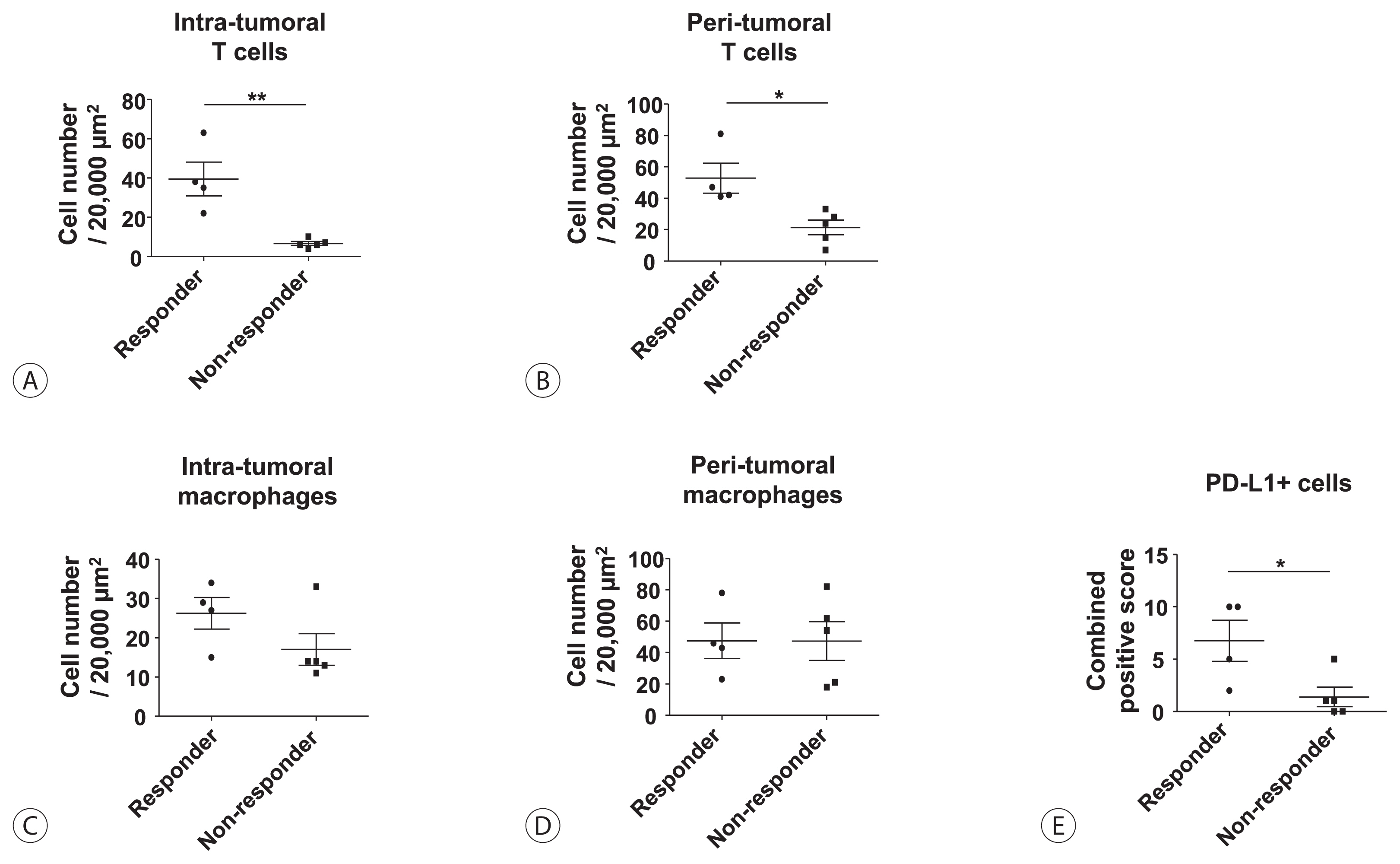
- Infiltration of T Cells and Programmed Cell Death Ligand 1-expressing Macrophages as a Potential Predictor of Lenvatinib Response in Hepatocellular Carcinoma
- Pil Soo Sung, Sung Woo Cho, Jaejun Lee, Hyun Yang, Jeong Won Jang, Si Hyun Bae, Jong Young Choi, Seung Kew Yoon
- J Liver Cancer. 2020;20(2):128-134. Published online September 30, 2020
- DOI: https://doi.org/10.17998/jlc.20.2.128
- 3,270 Views
- 98 Downloads
- 6 Citations
-
Abstract
PDF
- Background/Aim
s: Lenvatinib was recently proven to be non-inferior to sorafenib in treating unresectable hepatocellular carcinoma (HCC) in a phase-3 randomized controlled trial. In this study, we investigated whether the response to lenvatinib was affected by tumor immunogenicity.
Methods
Between May 2019 and April 2020, nine patients with intermediate-to-advanced HCC, who were treated with lenvatinib after liver biopsy, were enrolled. Immunohistochemical staining and multi-color flow cytometry were performed on specimens obtained from liver biopsy.
Results
Among the nine patients enrolled, four showed objective responses (complete responses+partial responses). Immunohistochemical staining for CD3, CD68, and programmed cell death ligand 1 (PD-L1) demonstrated that patients with objective responses showed marked infiltration of T cells and PD-L1-expressing macrophages in intra-tumoral and peri-tumoral tissues compared to those without objective responses. A significant difference in the numbers of infiltrated T cells, both in the intra-tumoral (P<0.01) and peri-tumoral regions (P<0.05), were identified between responders and non-responders. Regarding the number of infiltrated macrophages, no significant difference was found between the responders and non-responders, although the number of PD-L1-expressing tumor-associated macrophages was significantly higher in responders than that in non-responders (P<0.05).
Conclusions
Tumor immunogenicity, as indicated by T cell and PD-L1-positive macrophage infiltration, affects lenvatinib response in unresectable HCC. -
Citations
Citations to this article as recorded by
- Higher Number of Tumor-Infiltrating PD-L1+ Cells Is Related to Better Response to Multikinase Inhibitors in Hepatocellular Carcinoma
Ji Won Han, Ji Hoon Kim, Dong Hyun Kim, Jeong Won Jang, Si Hyun Bae, Jong Young Choi, Seung Kew Yoon, Jaegyoon Ahn, Hyun Yang, Pil Soo Sung
Diagnostics.2023; 13(8): 1453. CrossRef - Intrahepatic inflammatory IgA+PD-L1high monocytes in hepatocellular carcinoma development and immunotherapy
Pil Soo Sung, Dong Jun Park, Pu Reun Roh, Kyoung Do Mun, Sung Woo Cho, Gil Won Lee, Eun Sun Jung, Sung Hak Lee, Jeong Won Jang, Si Hyun Bae, Jong Young Choi, Jonghwan Choi, Jaegyoon Ahn, Seung Kew Yoon
Journal for ImmunoTherapy of Cancer.2022; 10(5): e003618. CrossRef - Crosstalk between tumor-associated macrophages and neighboring cells in hepatocellular carcinoma
Pil Soo Sung
Clinical and Molecular Hepatology.2022; 28(3): 333. CrossRef - Blood-based biomarkers for immune-based therapy in advanced HCC: Promising but a long way to go
Pil Soo Sung, Isaac Kise Lee, Pu Reun Roh, Min Woo Kang, Jaegyoon Ahn, Seung Kew Yoon
Frontiers in Oncology.2022;[Epub] CrossRef - Immunological Mechanisms for Hepatocellular Carcinoma Risk after Direct-Acting Antiviral Treatment of Hepatitis C Virus Infection
Pil Soo Sung, Eui-Cheol Shin
Journal of Clinical Medicine.2021; 10(2): 221. CrossRef - Preferential Expression of Programmed Death Ligand 1 Protein in Tumor-Associated Macrophages and Its Potential Role in Immunotherapy for Hepatocellular Carcinoma
Dong-Jun Park, Pil-Soo Sung, Gil-Won Lee, Sung-Woo Cho, Sung-Min Kim, Byung-Yoon Kang, Won-Hee Hur, Hyun Yang, Soon-Kyu Lee, Sung-Hak Lee, Eun-Sun Jung, Chang-Ho Seo, Joseph Ahn, Ho-Joong Choi, Young-Kyoung You, Jeong-Won Jang, Si-Hyun Bae, Jong-Young Cho
International Journal of Molecular Sciences.2021; 22(9): 4710. CrossRef
- Higher Number of Tumor-Infiltrating PD-L1+ Cells Is Related to Better Response to Multikinase Inhibitors in Hepatocellular Carcinoma
Case Reports
- Successful Sequential Therapy Involving Regorafenib after Failure of Sorafenib in a Patient with Recurrent Hepatocellular Carcinoma after Liver Transplantation
- Soon Kyu Lee, Jeong Won Jang, Heechul Nam, Pil Soo Sung, Si Hyun Bae, Jong Young Choi, Seung Kew Yoon
- J Liver Cancer. 2020;20(1):84-89. Published online March 31, 2020
- DOI: https://doi.org/10.17998/jlc.20.1.84

- 3,341 Views
- 89 Downloads
-
Abstract
PDF
- The efficacy and safety of sequential systemic therapy for the treatment of recurrent hepatocellular carcinoma (HCC) after liver transplantation (LT) are not well established. This study describes a successful experience where sequential therapy with sorafenib followed by regorafenib was used to treat recurrent HCC in a 54-year old male LT recipient. After HCC recurred in both lungs 10 months after LT, sorafenib was administered with radiation therapy to treat pulmonary metastases. However, after 4 months of sorafenib treatment showed progressive pulmonary metastases, sequential regorafenib treatment was started. After 3 months (cycles) of regorafenib treatment, tumor response was partial, and after 6 months (cycles), disease status remained stable without signs of progression or drug-related serious adverse events. This case suggests that sequential systemic therapy is feasible in patient with recurrent HCC after LT.
- Liver Transplantation after Successful Downstaging with Hepatic Arterial Infusion Chemotherapy in a Patient with Hepatocellular Carcinoma with Portal Vein Tumor Thrombus
- Hee Chul Nam, Pil Soo Sung, Ho Jong Chun, Dong Goo Kim, Jeong Won Jang, Jong Young Choi, Seung Kew Yoon
- J Liver Cancer. 2019;19(1):64-68. Published online March 31, 2019
- DOI: https://doi.org/10.17998/jlc.19.1.64

- 3,247 Views
- 58 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) is one of the most common cancers worldwide. The majority of patients with HCC are diagnosed at advanced disease stages with vascular invasion, where curative approaches are often not feasible. Currently, sorafenib is the only available standard therapy for HCC with portal vein tumor thrombosis (PVTT). However, in many cases, sorafenib therapy fails to achieve satisfactory results in clinical practice. We present a case of advanced HCC with PVTT that was treated with hepatic arterial infusion chemotherapy (HAIC) followed by liver transplantation. Three cycles of HAIC treatment resulted in necrotic changes in most of the tumors, and PVTT was reduced to an extent at which liver transplantation was possible. Further studies are required to determine the treatment strategies for advanced HCC with PVTT that can improve prognosis.
Original Article
- High-level Expression of Interleukin-17 and C-reactive Protein Predicts Tumor Progression in Unresectable Hepatocellular Carcinoma Treated by Transarterial Chemoembolization
- Myeong Jun Song, Sung Won Lee, Eun-Jee Oh, Bohyun Jang, Jeong Won Jang, Si Hyun Bae, Jong Young Choi, Seung Kew Yoon
- J Liver Cancer. 2016;16(2):108-117. Published online September 30, 2016
- DOI: https://doi.org/10.17998/jlc.16.2.108
- 949 Views
- 9 Downloads
-
Abstract
PDF
- Background/Aim
s: Transarterial chemoembolization (TACE) is the standard locoregional treatment in patients with unresectable hepatocellular carcinoma (HCC). Angiogenesis and inflammation play important roles in tumor growth in HCC. In this study, we evaluated the associations between the levels of growth factors and inflammatory markers and clinical prognosis in patients with unresectable HCC treated with TACE.
Methods
The clinical outcomes of 58 HCC patients treated with TACE at the Catholic Medical Centers from January, 2012 to February 2015 were evaluated. Baseline levels of the growth factors vascular endothelial growth factor, fibroblast growth factor, platelet-derived growth factor, and hepatocyte growth factor and the inflammatory cytokines interleukin (IL)-17 and high sensitivity C-reactive protein (hs-CRP) were compared with the treatment outcomes. The primary endpoint was time to progression (TTP); the secondary endpoint was overall survival (OS).
Results
During the 20.8 months of follow-up, TTP was significantly delayed in patients with low levels of hs-CRP (≤0.15) and IL-17 (≤0.94) and a maximal tumor diameter ≤5 cm (P =0.010, P =0.015, and 0.048, respectively). Patients with HCC with low hs-CRP and IL-17 levels had a longer survival than that of those with high hs-CRP levels and IL-17 (35.1 vs. 22.5 months, P =0.000; 41 vs. 21.8 months, P =0.000, respectively). However, any baseline growth factors were not significantly correlated with TTP and OS.
Conclusions
Elevated IL-17 and hs-CRP may be predictive of a poor outcome in patients with HCC treated with TACE. A better understanding of this relationship will require further investigation of the immune mechanisms underlying tumor progression.
Case Reports
- A Case of Complete Response by Multidisciplinary Management in a Patient with Solitary Bone Metastasis after Curative Resection of Hepatocellular Carcinoma
- Seawon Hwang, Hyun Yang, Hae Lim Lee, Jeong Won Jang, Si Hyun Bae, Jong Young Choi, Seung Kew Yoon
- J Liver Cancer. 2016;16(1):52-56. Published online March 31, 2016
- DOI: https://doi.org/10.17998/jlc.16.1.52
- 1,016 Views
- 12 Downloads
-
Abstract
PDF
- Despite recent advances in the treatment of hepatocellular carcinoma (HCC), the prognosis of patients with extrahepatic metastasis from HCC still remains dismal. The current study presents a case of HCC that was metastatic to the pelvis and describes successful treatment with multidisciplinary approach to the skeletal metastasis. The patient was a 67-year-old male who presented with right pelvic pain 28 months following right hepatectomy for HCC. Computed tomography and magnetic resonance imaging indicated a solitary bone metastasis without intrahepatic recurrence. Complete response was achieved with multidisciplinary management including sorafenib, transarterial embolization, surgery to remove the metastatic mass and radiotherapy after surgery. A post-operative follow-up 15 months later found that the patient remained in good health with maintained complete response. This case suggests that a multidisciplinary approach can achieve long-term cancer-free survival and prolonged life expectancy beyond palliative care for patients with solitary bone metastasis after curative surgery for HCC.
- A Case of Combination Therapy Using Radioembolization and Transarterial Chemoembolization with Drug-eluting Beads in Bilobar Hepatocellular Carcinomas
- Hee Yeon Kim, Chung-Hwa Park, Do Seon Song, Myeong Jun Song, Jong Young Choi, Seung Kew Yoon, Si Hyun Bae, Ho Jung Chun
- Journal of the Korean Liver Cancer Study Group. 2012;12(2):128-132. Published online September 30, 2012
- 514 Views
- 1 Download
-
Abstract
PDF
- Bilobar multifocal hepatocellular carcinomas (HCCs) can be treated with transarterial radioembolization in a sequential lobar, or whole liver manner. However, radioembolization could result in a risk of radiation-induced liver toxicity in patients with reduced functional reserve. Here we describe a case with bilobar HCCs successfully treated with a combination therapy using radioembolization and transarterial chemoembolization with drug-eluting beads without significant side effects. A 72-year-old female with liver cirrhosis was diagnosed of hepatocellular carcinoma with bilobar involvement. The main mass in the left lobe was treated with radioembolization while the other lesion in the right lobe was treated with transarterial chemoembolization using drug-eluting beads, and the patient was tolerable. A combination of radioembolization and selective transarterial chemoem- bolization may be considered for an alternative option in patients with bilobar multifocal HCCs with decreased liver function.
- A Case of Hepatocellular Carcinoma which Showed Response to Transarterial Chemoembolization with DC Bead® in the Patient who Showed No Response to Conventional Transarterial Chemoembolization
- Do Seon Song, Hee Yeon Kim, Myeong Jun Song, Si Hyun Bae, Jong Young Choi, Seung Kew Yoon, Ho Jong Chun
- Journal of the Korean Liver Cancer Study Group. 2012;12(2):133-136. Published online September 30, 2012
- 523 Views
- 1 Download
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) is one of the most important cause of cancer death in South Korea. Approximately two thirds of the HCC patients are diagnosed in the unresectable stage. Conventional transarterial chemoembolization (TACE) showed survival benefit in the unresectable HCC patients, but it had some limitations, such as low response rate and systemic toxicity. Drug eluting bead has been reported low systemic toxicity and higher tumor necrosis rate. We report a case which showed response to TACE with DC bead in patient that showed no response to conventional TACE.
- A Case of Hepatocellular Carcinoma in a 10 Year Old Child Treated with Yttrium Radioembolization and Transarterial Chemoembolization
- Sung Won Lee, Hee Yeon Kim, Do Seon Song, Chung-Hwa Park, Myeong Jun Song, Jong Young Choi, Seung Kew Yoon, Jung Suk Oh, Ho Jong Chun, Si Hyun Bae
- Journal of the Korean Liver Cancer Study Group. 2012;12(2):137-140. Published online September 30, 2012
- 533 Views
- 4 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) in childhood is rare but is the second most common malignant liver neoplasm after hepatoblastoma in children. Surgical resectability is the foundation of curative therapy but only one third of newly diagnosed HCCs are resectable, and unresectable HCC remains largely unresponsive to systemic chemotherapy. In all reported series of HCC in children, therapeutic results are poor with overall survival less than 30%. Systemic chemotherapy is only partially effective but if preoperative downstaging can be achieved, it would result in a higher survival rate. There are scarce data regarding local ablative treatments such as transarterial chemoembolization (TACE) and therefore survival benefits are still unclear. TACE may be considered as a therapeutic alternative in cases of unresectable tumors after systemic chemotherapy or in unresectable, non-metastatic HCCs. The use of orthotopic liver transplantation in childhood HCC remains controversial. Radioembolization is a mode of treatment that aims to selectively target radiation to all liver tumors using yttrium-90 microspheres while limiting the dose to normal liver parenchyma. It may be considered as another treatment option in childhood HCC with the purpose of preoperative downstaging but further studies are required to determine the treatment benefits and safety of radioembolization treatment.
- A Case of Progressive Superior Mesenteric Vein Thrombosis after Percutaneous Transhepatic Obliteration in Infiltrative Hepatocellular Carcinomaswith Portal Vein Thrombosis
- Hee Yeon Kim, Chung-Hwa Park, Sung won Lee, Do Seon Song, Myeong Jun Song, Jong Young Choi, Seung Kew Yoon, Si Hyun Bae, Jung Suk Oh, Ho Jong Chun
- Journal of the Korean Liver Cancer Study Group. 2012;12(2):146-150. Published online September 30, 2012
- 524 Views
- 3 Downloads
-
Abstract
PDF
- Percutaneous transhepatic obliteration of gastroesophageal varices is one of the effective emergency procedure when endoscopic therapy is not indicated or has been failed. One of the major complications of this procedure is portal thrombosis. A 53-year-old male with hepatitis B virus infection was diagnosed of infiltrative hepatocellular carcinoma with right portal vein thrombosis. On the next day after being hospitalization, the patient developed variceal bleeding. With medical management, endoscopic therapy was initially attempted, however, it ended in failure. Emergency percutaneous transhepatic obliteration of bleeding gastroesophageal varices was considered as a next option. Bleeding from gastroesophageal varices was stopped after percutaneous obliateration, however, portal thrombosis was extended to splenic vein or superior mesenteric veins.
- A Case of Liver Transplantation after Combination of Sorafenib and Hepatic Arterial Infusion Chemotherapy in the Advanced Hepatocellular Carcinoma Patient with Portal Vein Thrombosis
- Do Seon Song, Myeong Jun Song, Si Hyun Bae, Jong Young Choi, Seung Kew Yoon, Ho Jong Chun, Dong Goo Kim
- Journal of the Korean Liver Cancer Study Group. 2012;12(1):62-66. Published online February 28, 2012
- 610 Views
- 0 Download
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) is the third most common malignancy in Korea where chronic hepatitis B virus is prevalent. More than 60-70% of HCC cases are diagnosed at an advanced stage that are not eligible for curative therapy such as surgical resection, liver transplantation, radiofrequency ablation, and percutaneous ethanol injection. According to Barcellona Clinic Liver Cancer (BCLC) staging and treatment, standard treatment of advanced HCC is sorafenib. And there are some reports that hepatic arterial infusion chemotherapy (HAIC) could be a beneficial therapeutic option for patients with advanced HCC. We report a case of advanced HCC with portal vein thrombosis that received liver transplantation after combination treatment of HAIC and sorafenib.
- Conus Medullaris Syndrome after Transcatheter Arterial Chemoembolization in Patient with Hepatocellular Carcinoma
- Sun Hong Yoo, Si Hyun Bae, Pil Soo Sung, Hee Yeon Kim, Do Seon Song, Myeong Jun Song, Jong Young Choi, Seung Kew Yoon, Ho Jong Chun
- Journal of the Korean Liver Cancer Study Group. 2011;11(2):185-189. Published online September 30, 2011
- 585 Views
- 7 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) is the fourth most common cancer in Korea and a common cause of cancer death. Transcatheter arterial chemoembolization (TACE) is used as palliative therapy for patients with inoperable HCC. TACE is an effective treatments for inoperable HCC, but variable complications due to using embolic agents can occur after TACE. Complications due to embolic agents include pulmonary lipiodol embolism, splenic infarction, cerebral lipiodol infarction, and spinal cord injury. This is a rare case of spinal cord injury after a sixth TACE via right T9 intercostal artery.
- From Down Staging to Curative Treatment: Based on Hepatic Arterial Infusion Chemotherapy in a Hepatocellular Carcinoma Patient
- Chung-Hwa Park, Myung Joon Song, Seung Kew Yoon, Jong Young Choi, Si Hyun Bae
- Journal of the Korean Liver Cancer Study Group. 2011;11(1):46-49. Published online February 28, 2011
- 545 Views
- 1 Download
-
Abstract
PDF
- Hepatic arterial infusion chemotherapy (HAIC) is performed in patients with advanced hepatocellular carcinoma (HCC) in which locoregional therapeutic methods such as transarterial chemoembolization (TACE), percutaneous ethanol injection (PEI) or radiofrequency ablation (RFA) could not be the best choice. Sorafenib, the only approved systemic chemotherapeutic agent for HCC, improves survival rate, but is associated with a low tumor response rate. Thus combining these therapeutic modalities to treat HCC in advanced stage may help downstaging and leading to better treatment results without taking risk for hepatic failure. Here we report a case treated to a complete remission by combining HAIC, PEI and sorafenib.
 First
First Prev
Prev


 Follow JLC on Twitter
Follow JLC on Twitter